Case studies are great learning tools for coders, providing an array of detail and rationale to enhance understanding. Here, we explore a case study related to venous access for correct coding. By examining case studies like these, coders can ensure success throughout the year.
VENOUS ACCESS CASE: TUNNELED DIALYSIS CATHETER PLACEMENT
Clinical History: Adult patient with end-stage renal disease, difficult venous access, and nonfunctioning right groin arteriovenous (AV) graft needs intermediate-term central venous access for hemodialysis. The vascular surgeon is planning for a new AV graft in the left thigh. The referring nephrology service has asked for a tunneled dialysis catheter placement in the right groin.
Clinical History: Adult patient with end-stage renal disease, difficult venous access, and nonfunctioning right groin arteriovenous (AV) graft needs intermediate-term central venous access for hemodialysis. The vascular surgeon is planning for a new AV graft in the left thigh. The referring nephrology service has asked for a tunneled dialysis catheter placement in the right groin.
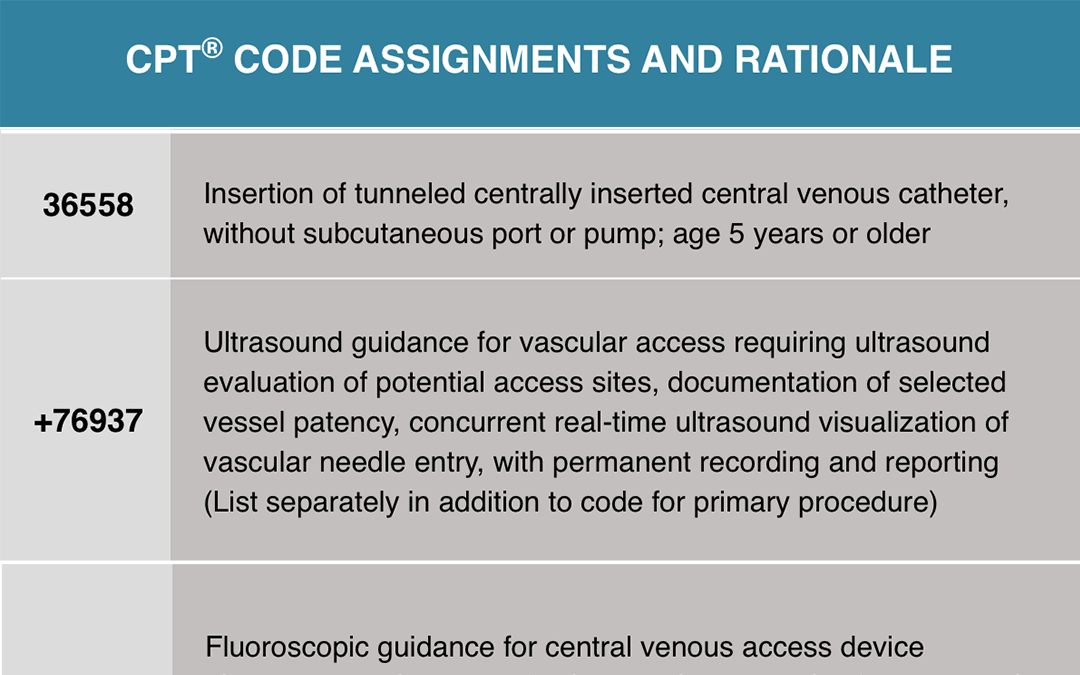
Procedure Performed: Right femoral tunneled hemodialysis catheter placement. The risks, benefits and alternatives to the procedure were explained to the patient, and informed written consent was obtained. The patient was brought to the interventional radiology suite where a time-out procedure was performed. The patient was placed in the supine position. The right groin was prepped and draped in the usual sterile fashion. Real-time ultrasound was used, and a permanent image stored. Using ultrasound guidance the right common femoral vein was punctured with a micropuncture needle, after infiltration of the skin and deep tissues with local anesthetic. A 50 cm tip to cuff length, 14.5-French dual lumen Vaxcel® hemodialysis catheter was inserted. The catheter was placed through a subcutaneous tunnel requiring a second incision. The incision at the femoral vein access site was closed with 4-0 Vicryl® suture. The catheter was secured at the skin exit site with 2-0 Prolene® suture. There is free aspiration of blood from all ports of the catheter, which were locked with heparin (concentration 1000 units/cc). A sterile dressing was then applied. Postprocedure chest fluoroscopy showed the tip of the catheter at the right atrium, and an image was stored in the medical record.
The pre-existing left femoral catheter was removed in its entirety. A sterile dressing was applied. The patient tolerated the procedure well with no immediate complications. This procedure was performed using ultrasound and fluoroscopy. Impressions:
- Ultrasound of the right groin demonstrates patent and compressible femoral vein.
- Successful right femoral tunneled hemodialysis catheter placement with its tip positioned at the right atrium as discussed above.
There is free aspiration of blood from all ports of the catheter. The catheter is ready for immediate use.
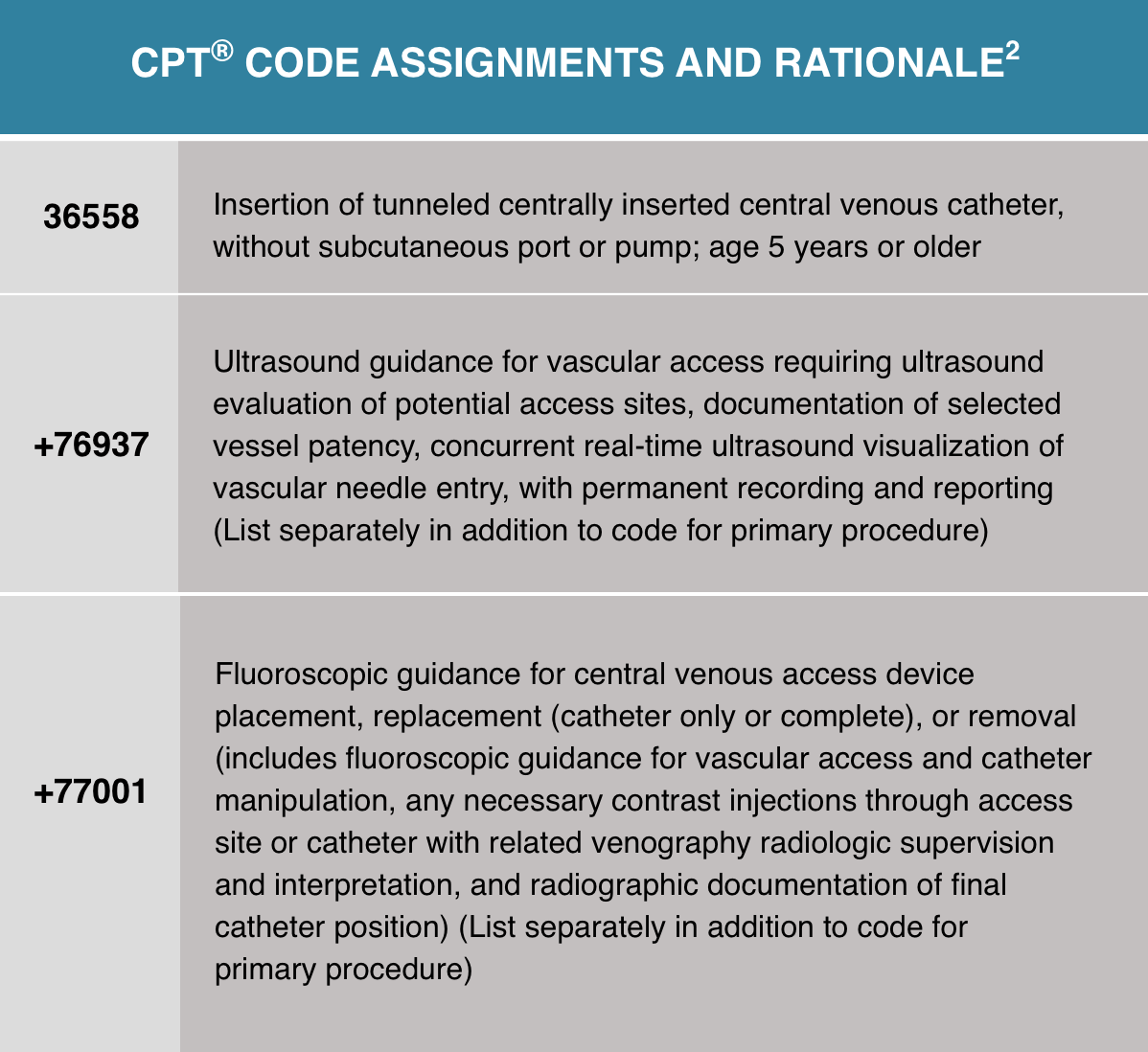
Ultrasound was used to locate a suitable vein and to guide the needle access into that vein. An image of the vein was obtained for a permanent record. A catheter was placed from a central vein (femoral vein) into the right atrium of the heart using fluoroscopic guidance including a permanent image of the final position. The catheter was tunneled from a skin entry site away from the vein.
Although the report documents that a previously existing catheter was removed, there is no documentation that it was a tunneled catheter or that dissection was required to remove it. Therefore, no removal code would be assigned.
References:
- Nordley, B. (2022, July 15). Venous Coding Case Example for Enhanced Understanding. MedLearn Publishing. https://medlearn.com/venous-coding-case-example-for-enhanced-understanding/
- American Medical Association. 2022 Professional Edition CPT® Current Procedural Terminology. Chicago, IL: American Medical Association; 2021.